No products in the cart.
Blog
Semaglutide vs Tirzepatide vs Retatrutide
Semaglutide vs Tirzepatide vs Retatrutide: The Complete Comparison
Three generations of GLP-1 treatment. One definitive guide — receptor mechanisms, Phase 3 data, side effect profiles, and exactly who each drug is right for.
{kind=link}
Three Generations of GLP-1 Treatment
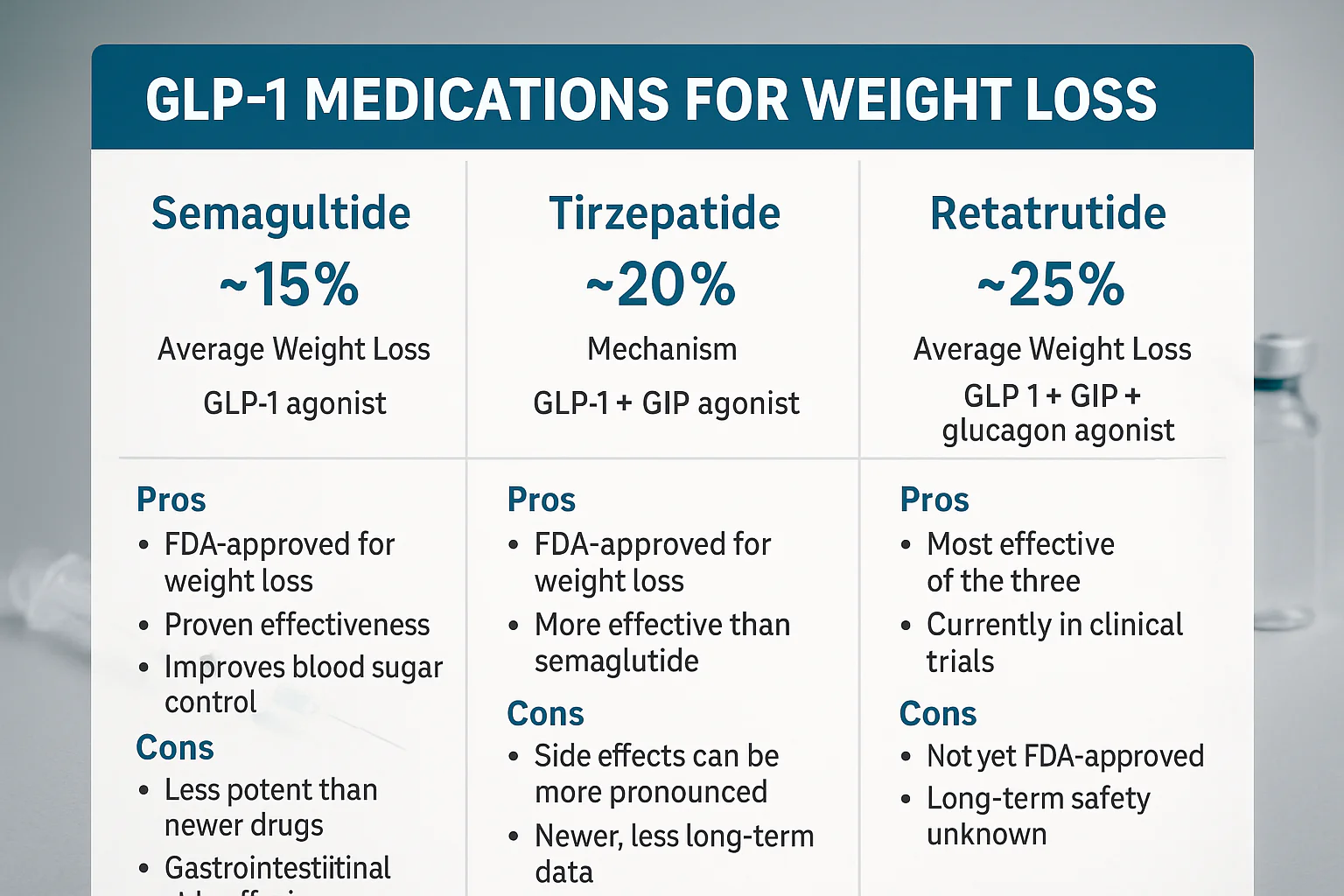
The evolution from semaglutide to tirzepatide to retatrutide represents the most rapid advancement in obesity pharmacology in history. Each generation adds receptor targets, and each addition translates directly into greater weight loss outcomes. Here is the headline picture before we go deep:
Generation 1
Semaglutide
GLP-1 receptor only
1 pathway activated
1 pathway activated
~15%
Avg. weight loss (STEP 1, 68 wks)
Generation 2
Tirzepatide
GLP-1 + GIP
2 pathways activated
2 pathways activated
~22.5%
Avg. weight loss (SURMOUNT-1, 72 wks)
Generation 3
Retatrutide
GLP-1 + GIP + Glucagon
3 pathways activated
3 pathways activated
~28.3%
Avg. weight loss (TRIUMPH-1, 80 wks)
All three drugs are available from Synedica UK. The choice of which to use — and in what order — depends on your treatment history, tolerance, and goals.
How Each Drug Works
Semaglutide — The GLP-1 Foundation
Synedica Semaglutide activates the GLP-1 (Glucagon-Like Peptide-1) receptor. GLP-1 slows gastric emptying, signals satiety to the brain, and stimulates insulin release in a glucose-dependent manner. Semaglutide was the first GLP-1 agonist to demonstrate sustained average weight loss exceeding 10% in a Phase 3 trial — a milestone that transformed the obesity treatment landscape. It remains the right first-line choice for new users due to its well-established safety record and extensive real-world data.
Tirzepatide — Adding the GIP Layer
Synedica Tirzepatide adds GIP (Glucose-Dependent Insulinotropic Polypeptide) receptor activation on top of GLP-1. GIP works synergistically with GLP-1 to enhance insulin secretion, regulate fat metabolism, and amplify energy balance effects. A 2025 meta-analysis of direct comparative studies (28,980 participants) confirmed tirzepatide’s superiority over semaglutide, with greater weight loss across all timepoints and a significantly higher proportion achieving 10%+ body weight reduction.
Retatrutide — The Triple Agonist
Synedica Retatrutide adds glucagon receptor activation to the GLP-1/GIP combination. Glucagon promotes energy expenditure and fat breakdown (lipolysis), particularly in the liver — adding a third metabolic lever that neither semaglutide nor tirzepatide can activate. This is why retatrutide produces the highest weight loss in clinical trials, and why it shows the most dramatic reduction in liver fat (MASLD). The glucagon component is also responsible for retatrutide’s unique side effects: dysesthesia and greater heart rate elevation.
🔬 Each generation doesn’t replace the previous one — it adds to it. Retatrutide still works through GLP-1 and GIP (the same pathways as semaglutide and tirzepatide), making it a natural next step rather than a fundamentally different mechanism.
Weight Loss Results: Phase 3 Data
Here is how the three drugs compare in their respective landmark Phase 3 trials. Note that these trials ran over slightly different durations and enrolled different populations, so the comparisons are directional rather than head-to-head:
| Trial | Drug | Top Dose | Duration | Avg. Weight Loss | ≥15% achieved |
|---|---|---|---|---|---|
| STEP 1 | Semaglutide | 2.4mg | 68 wks | ~14.9% | ~32% |
| SURMOUNT-1 | Tirzepatide | 15mg | 72 wks | ~22.5% | ~55–63% |
| TRIUMPH-1 | Retatrutide | 12mg | 80 wks | ~25–28.3% | Data pending |
A direct head-to-head comparison of retatrutide versus tirzepatide is currently underway in the TRIUMPH-5 trial (NCT06662383), expected to report results in late 2026 or early 2027. This will be the most definitive data for the two most advanced treatments. (Source: ClinicalTrials.gov)
Full Feature Comparison Table
| Feature | Semaglutide | Tirzepatide | Retatrutide |
|---|---|---|---|
| Receptors | GLP-1 (1) | GLP-1 + GIP (2) | GLP-1 + GIP + Glucagon (3) |
| Avg. weight loss (top dose) | ~15% | ~22.5% | ~25–28.3% |
| ≥30% weight loss achievable | Rare | ~39.7% (≥25%) | 45.3% (≥30%) |
| Liver fat reduction (MASLD) | Modest | Significant | Superior (86% normalisation) |
| Dosing frequency | Once weekly | Once weekly | Once weekly |
| Nausea (top dose) | ~44% | ~33% | ~43% |
| Dysesthesia | Not seen | Not seen | ~21% at 12mg |
| Heart rate increase | ~2–4 bpm | ~2–4 bpm | ~5–10 bpm |
| Real-world safety data | Extensive | Good | Limited (Phase 3) |
| Right for | New users | After sema tolerance | After tirz tolerance / advanced |
| Synedica product | Semaglutide pen → | Tirzepatide pen → | Retatrutide pen → |
Side Effects Compared
All three drugs share the same family of gastrointestinal side effects — this is inherent to GLP-1 receptor activation and not specific to any individual drug. The differences lie in frequency, and in retatrutide’s two unique effects.
GI effects: Semaglutide tends to have the highest GI burden at its top dose (nausea ~44%). Tirzepatide’s dual mechanism is somewhat better tolerated (~33% nausea). Retatrutide’s nausea rate (~43%) is comparable to semaglutide despite delivering substantially greater weight loss. All three drugs’ GI side effects peak during dose escalation and settle at maintenance.
Dysesthesia: Unique to retatrutide. Affecting ~21% of users at 12mg in Phase 3 TRIUMPH-4. Generally mild, rarely causes discontinuation, typically resolves by week 24. Not seen with semaglutide or tirzepatide at any dose.
Heart rate: Semaglutide and tirzepatide raise resting heart rate by approximately 2–4 bpm. Retatrutide raises it 5–10 bpm, peaking around week 24 then declining. This is a consideration for users with cardiovascular risk factors.
Gallbladder: Tirzepatide shows the highest rates of gallbladder-related events across the three drugs. Rapid weight loss from any drug increases gallstone risk; tirzepatide’s particular mechanism appears to amplify this.
⚠️ Safety context: semaglutide has the longest and most extensive real-world safety record of the three, with years of post-approval data. Tirzepatide has several years of post-approval data. Retatrutide remains investigational — its long-term safety profile beyond 80 weeks is genuinely unknown, not merely unstudied.
Who Each Drug Is Right For
Start with Semaglutide if…
- You are completely new to GLP-1 therapy
- You want the most established safety record with years of real-world data
- Your goal is clinically meaningful weight loss without maximising receptor coverage from the outset
- You are GI-sensitive and want the gentlest entry point
Progress to Tirzepatide if…
- You have used semaglutide at higher doses and reached a weight loss plateau
- You want to add GIP receptor activation for enhanced glucose and fat metabolism effects
- You are seeking meaningfully greater weight loss than semaglutide can deliver (22.5% vs 15%)
- You have type 2 diabetes alongside obesity — the GIP component enhances glucose control
Advance to Retatrutide if…
- You have used tirzepatide at higher doses and plateaued, or developed tolerance
- You want the highest weight loss ceiling currently available in a once-weekly injectable
- You have elevated liver fat (MASLD) and want glucagon-mediated liver fat reduction
- You have severe obesity (BMI ≥35) and are seeking bariatric-level results without surgery
The Synedica Progression Protocol
The clinical guidance endorsed by Synedica — and consistent with Phase 3 trial design — is a step-up approach. This is not arbitrary; it reflects how receptor tolerance develops and how each drug’s mechanism builds on the previous one.
💡 Not everyone needs to reach Step 3. Many users achieve their goals at Step 1 or Step 2. The protocol is a ceiling, not a prescription — use the lowest step at which you are achieving consistent progress and good tolerability.
⚠️ All treatment decisions — including which drug to start with, when to progress, and at what dose — should be made with a qualified healthcare provider who can monitor your response and manage any side effects.
Frequently Asked Questions
Which is the most effective: semaglutide, tirzepatide or retatrutide?
By average weight loss in Phase 3 trials: retatrutide (25–28.3%) > tirzepatide (22.5%) > semaglutide (~15%). However, “most effective” depends on your individual response and tolerance. Some users achieve outstanding results on semaglutide alone; others need the additional receptor coverage. The step-up protocol matches you to the lowest-level drug that delivers your goal.
Can I start with retatrutide without using semaglutide or tirzepatide first?
In principle, yes — some patients with severe obesity (BMI ≥40) and significant comorbidities may be directed to retatrutide from the outset by their provider. However, the standard guidance is to start with semaglutide to establish GLP-1 tolerance before progressing. This reduces side effect burden and allows you to identify your individual response profile before moving to the more potent triple agonist.
Is tirzepatide or semaglutide better for type 2 diabetes?
Both are clinically effective for type 2 diabetes. Tirzepatide’s additional GIP activation provides enhanced glucose control — direct comparison data (SURPASS-2) showed tirzepatide delivering superior A1C reduction versus semaglutide at all doses. Retatrutide’s TRANSCEND-T2D-1 Phase 3 trial also showed up to 2.0% A1C reduction, making it highly competitive for diabetic patients alongside its obesity benefits.
All Three Products Available at Synedica UK
Whether you’re starting with semaglutide or advancing to retatrutide, all three Synedica pen kits ship free on every order.
Sources & References
- Eli Lilly. TRIUMPH-1 Phase 3 Results. May 2026. prnewswire.com
- Eli Lilly. SURMOUNT-1 — Tirzepatide 22.5% weight loss. NEJM, 2022. investor.lilly.com
- Wilding et al. STEP 1 — Semaglutide 14.9% weight loss. NEJM, 2021.
- NCT06662383 — TRIUMPH-5 head-to-head trial. clinicaltrials.gov
- Lola Health. Retatrutide vs Semaglutide vs Tirzepatide comparison. 2026. lolahealth.com
- PubMed. Tirzepatide vs Semaglutide — Meta-Analysis. 2025. ncbi.nlm.nih.gov